
In my 38 years in behavioral health, I have been written up by a supervisor only once, and that was for… you guessed it: documentation. The first organization I worked for had a policy requiring all progress notes to be written and submitted to our clerical staff within 48 hours of the service provided. Well, let’s just say, it took me a little longer than that. Initially, I was upset about it. Couldn’t they just be happy with all the great work I was doing? I mean, case management is hard work, and I was seeing a lot of people each day working with a challenging population. Plus, I didn’t get into this field to do documentation; I got into this field to help people!
Once my internal defensive rant subsided, I was able to refocus and listen to my supervisor, who was actually an incredibly nice and supportive person. She helped me recognize the internal fight I was having with documentation and how it was making the task more burdensome than it needed to be. She picked out a set of my recent progress notes from one chart and then prompted me to walk through what I had been working on with the person and how it went.
Together, we concluded that I was trying to recreate everything in my progress note that happened in a session, and I was trying too hard to create a note that I thought an auditor wanted to read, rather than simply telling the story of the efforts being made to help the person receiving services progress toward their goals. In short, I was taking too much time to write one note, started feeling overwhelmed with all the notes I had to write, and then put it off to the next day. Only to find, the next day was overwhelming, and…you get the point.
In this blog, what I hope to accomplish is to help you become better friends with progress note writing (or at least not dreaded enemies). I will draw from what I learned from my supervisor, who helped me substantially improve my note-writing skills, along with my own learning over the years. While each organization has its own requirements for documentation that align with the expectations of its funding sources (which are essential to adhere to), I will show how to write notes that are completely aligned with Strengths Model practice AND have been able to stand the test of time, meeting the requirements of any behavioral health quality assurance department I have encountered.
Why Document Anything?
This is an important question to answer before we begin. For starters, it is essential. It ensures that programs get paid for the work you do (which supports you getting paid – win-win). It provides accountability that the services being provided are justified within the person’s overall plan of care. It also supports communication and continuity of care by ensuring that all providers involved in the person’s care work together to support the person’s progress. And while all of these things are important, there is also more to it that benefits the worker and the person receiving services. It can be a way for the worker to remain self-reflective about their practice and to continuously ground their work in helping people identify, clarify, and make progress toward meaningful and important life goals. Quite simply, good documentation has the potential to tell the ongoing story of the helping relationship.
What Progress Note Format to Use?
There are several progress note formats used in behavioral health (GIRP, PIRP, BIRP, DAP, SOAP, just to name a few). While most of us don’t get to choose which format our organizations use for progress notes, I have found GIRP (Goal, Intervention, Response, Plan) to be most aligned with writing notes for Strengths Model Case Management. This is because it keeps the mutually identified goal that the worker and client are working toward together in the session at the top of the note (or efforts to engage and identify goals in the early engagement and planning phase of services). Since SMCM is a recovery-oriented, goal-driven practice, this helps to shape the remainder of the note. Intervention is what the worker and client did during the session related to the goal, including any specific therapeutic techniques, strategies, or tools used. Response records the client’s observable reactions to the intervention, including any progress noted. Plan outlines the next steps for service provision, including any specific actions the worker or client will take before the next session.
I have found that many funders also prefer GIRP because when aligned with a clear and specific Care Plan (or Treatment Plan), it transparently shows that the services provided are intentionally focused on moving toward something that will improve the well-being of the person receiving services (and successfully transitioning out of services).
When to Start the Progress Note
I have found that the best time to start a progress note is right before a session even starts. What? You can’t start a note before you do anything! I disagree. While you can’t write what happens in a session before it occurs, part of being a skilled Strengths Model case manager is being intentional and purposeful in the work you do with people, not merely reactionary. So, what I did right before I started a session with a person is I divided up the upper three-fourths of a blank sheet in my notebook into four quadrants. Each quadrant represented something important that would eventually go into my future progress note. The top left quadrant was for the goal that the person and I planned on working toward that day, the bottom left was for what we actually did in that session related to the goal, the upper right quadrant was to record how the person responded to what we did that day along with any key results, and the bottom right quadrant was to record next steps for the next session or anything that we agreed to do between sessions. In the bottom fourth of the page, I left room to record any important observations I noted during the session or any miscellaneous notes that didn’t seem to fit into any of the quadrants at the top of the page. Figure 1 shows what this looked like on my notepad.
Figure 1: Template for Recording Information for Progress Note During Session
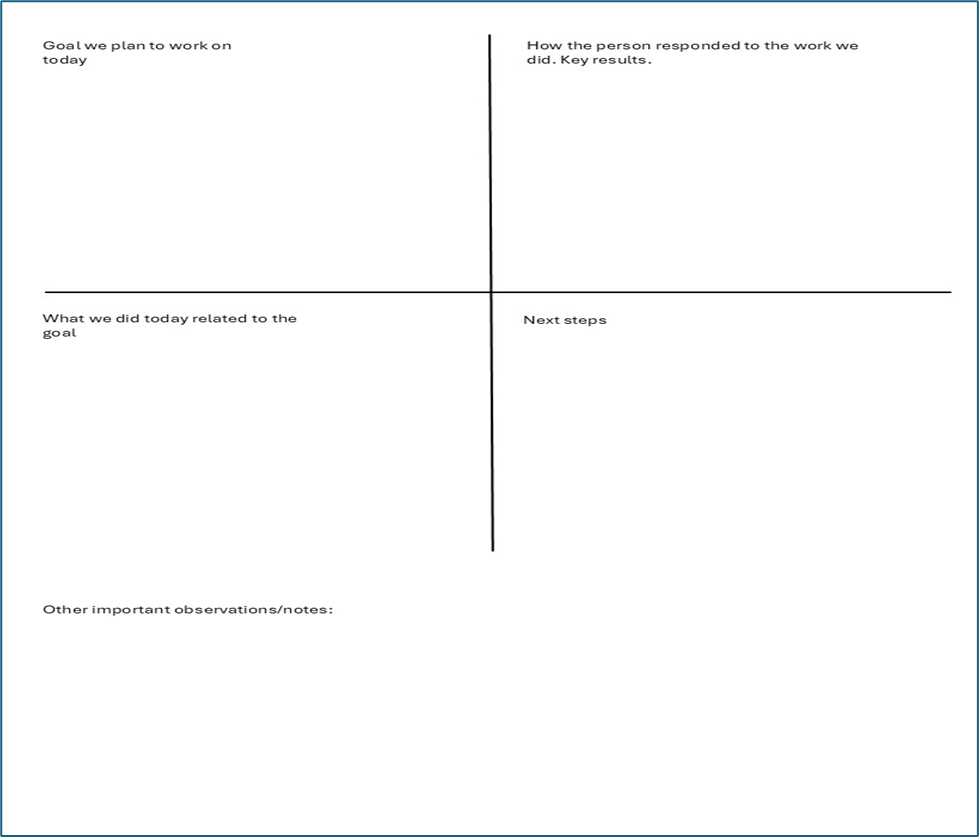
Initially, I would title each section as shown in Figure 1. Eventually, I would just quickly draw the quadrants, knowing what would go into each section. The only thing I would write in the quadrants before the session was the goal or goals I planned to work on with the person that day. This would help me to get grounded in what was truly meaningful and important to the person and what we agreed to work toward in their Treatment Plan. Now, I know what you are thinking. Sometimes, things change rapidly in our work with people, and what we plan to work on doesn’t always occur. Crises happen, or there is an immediate need that needs to be responded to that day. That’s fine. We can take care of anything within a session that needs to be addressed. Being mindful of the goal we intend to work on keeps us grounded in the overall plan of care, which hopefully was developed using the client-centered approach of the Strengths Assessment. If a particular session requires us to deviate from that plan, then this can be reflected in our final progress note, along with our plan to resume working on the goal, if this is something the person still wants to work toward.
Once our session begins, we can use the template to record any activities, observations, interventions, results, and a summary of agreed-upon next steps. In the spirit of trauma-informed, transparent services, I let the person see the template I use and let them know that I will be using it to take notes for their chart record. They are even welcome to see what I write at any time. In fact, it helps, in the spirit of collaborative documentation, which I will discuss later. Figure 2 is an example of notes taken using the template for a person whose goal is to get a job. Taking steps has been challenging for this person due to experiencing anxiety and easily getting overwhelmed. The information in the template is typed, though in practice, you would just handwrite it. It’s not essential that you capture everything that is said in the session. In fact, that’s the point. The template is to help you stay focused on the key points that will eventually make it into your progress notes.
Figure 2. Completed Template for Recording Information for a Progress Note
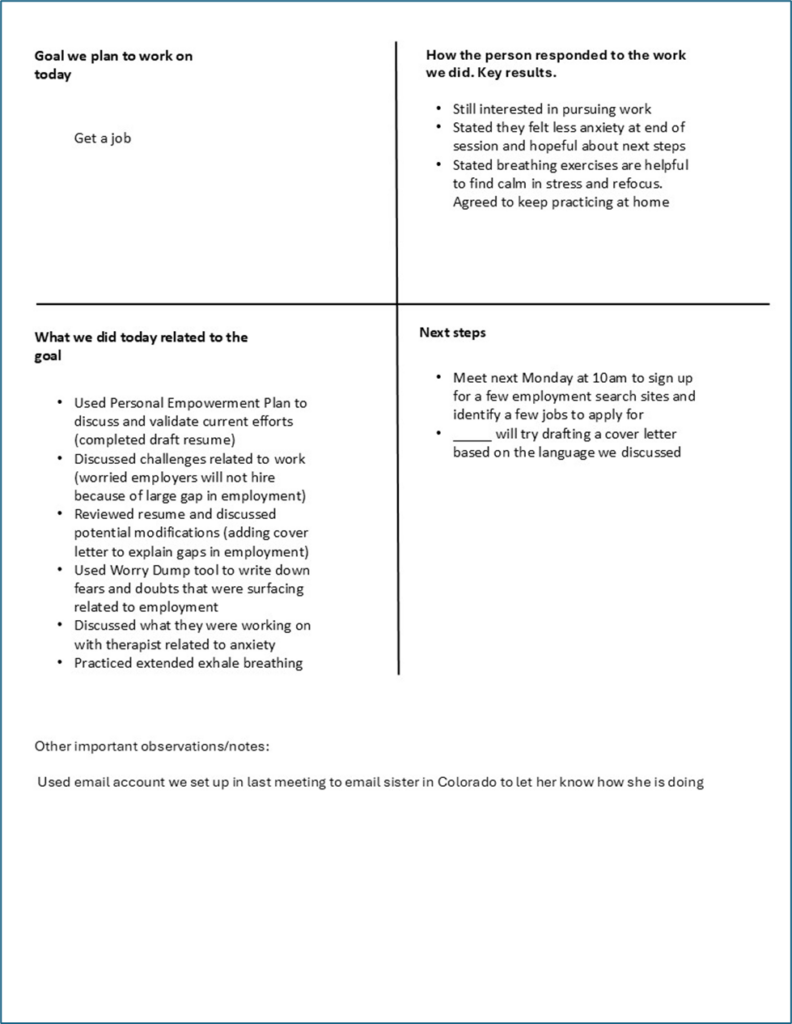
I like to think of it as separating the “news” from the “noise.” If the person talked for a few minutes about a new TV show they were watching or an unpleasant encounter they had at the grocery store, you get to decide whether this is just a conversation that occurred within the session or something important to note related to what you were working on that day. It’s also not important how much you write on the template (if you decide to use it). Sometimes, the steps you are taking require you to be out in the community completing actual tasks, and it isn’t always easy to write things down. It’s okay to jot a few things down at the end of the session to jog your memory for the progress note, or, if you have time, discuss the session with the person toward the end to summarize what you did that day and plan next steps.
Remember why you are doing this. It’s not to create additional documentation; it’s to help you more easily recall, remain focused, and complete the documentation you do need to complete.
Writing the Progress Note
If you captured the correct information in the note template, writing the progress note should be fairly straightforward. Here I will write a progress note in GIRP format using the information collected in Figure 2.
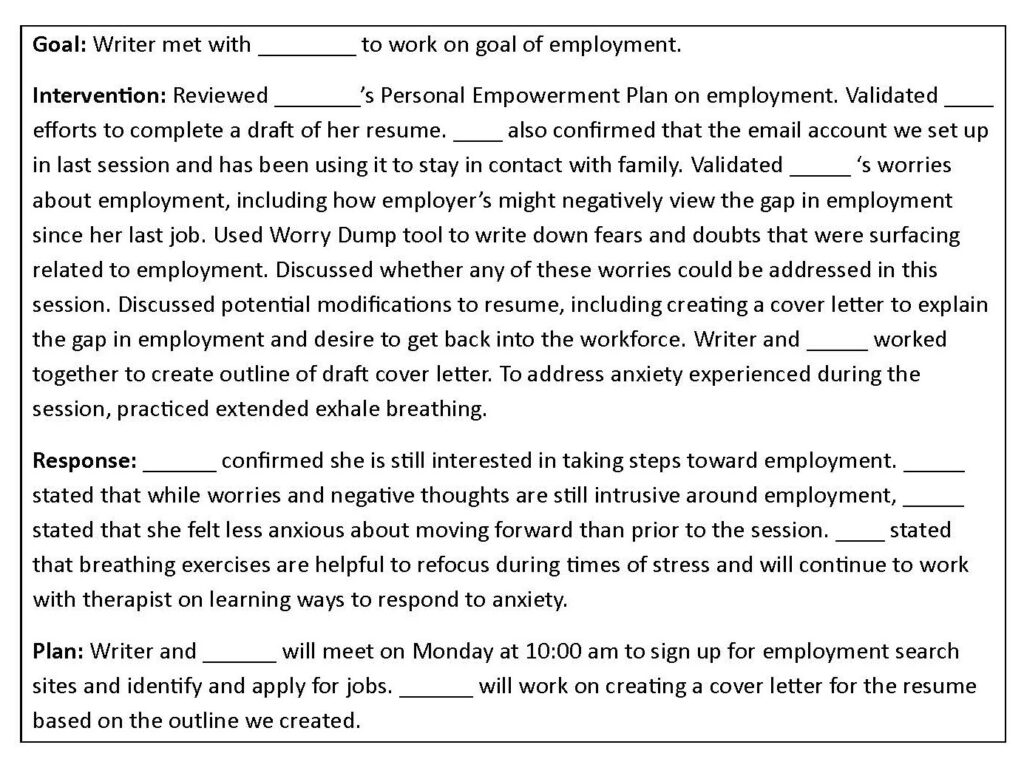
I found that when I used the above template to take notes during a session, I could write most progress notes in 5-10 minutes. I found the same to be true of the people I supervised, whom I taught this process.
What if the session deviates from the goal we planned to work on?
Ok, well, maybe when things go smoothly in a session, working on a specific goal, like in your example above. What about when things deviate from the plan, and you have to take care of an unforeseen problem that arises? Let’s take the same scenario above and imagine that when we arrived at the person’s apartment to work on their employment goal, the person stated that they were experiencing severe tooth pain. Figure 3 shows how using the template might look.
Figure 3. Completed Template for Recording Information for Progress Note (Deviation from goal)
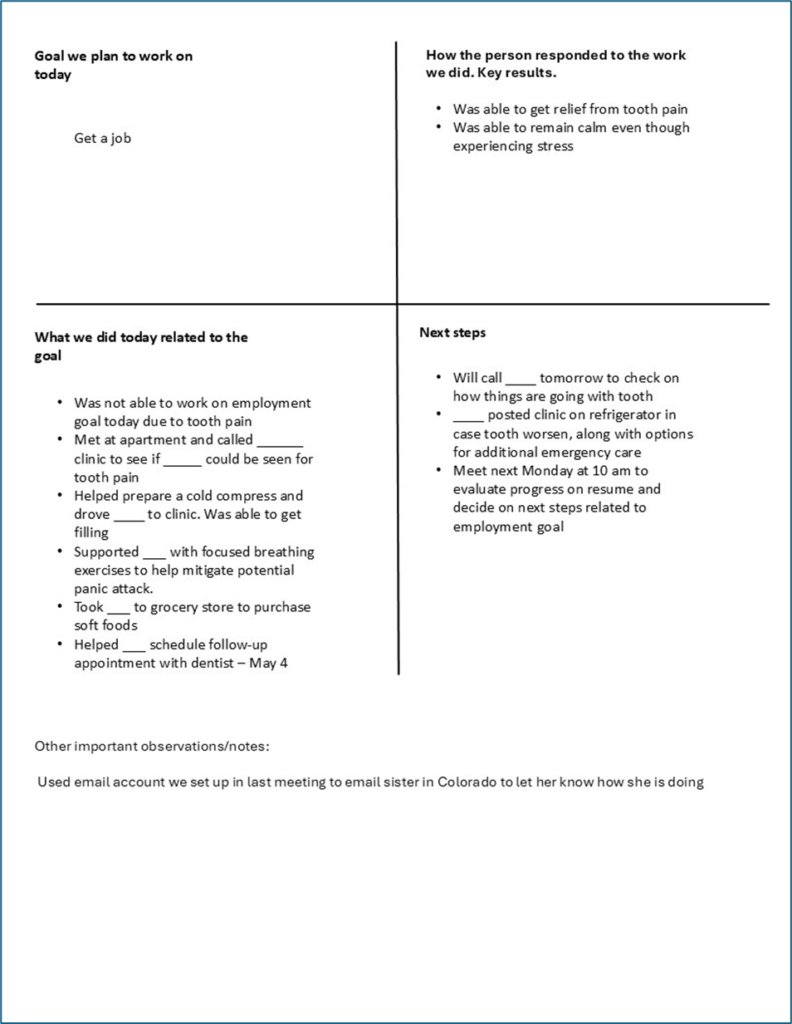
As with the last example, we still start by writing the goal we intended to work on that day (employment) in the upper-left quadrant. While what we did in the session changed due to the circumstances, we return to focus again on the employment goal in the next steps section written in the lower right quadrant. Below is an example of what that progress note might look like.
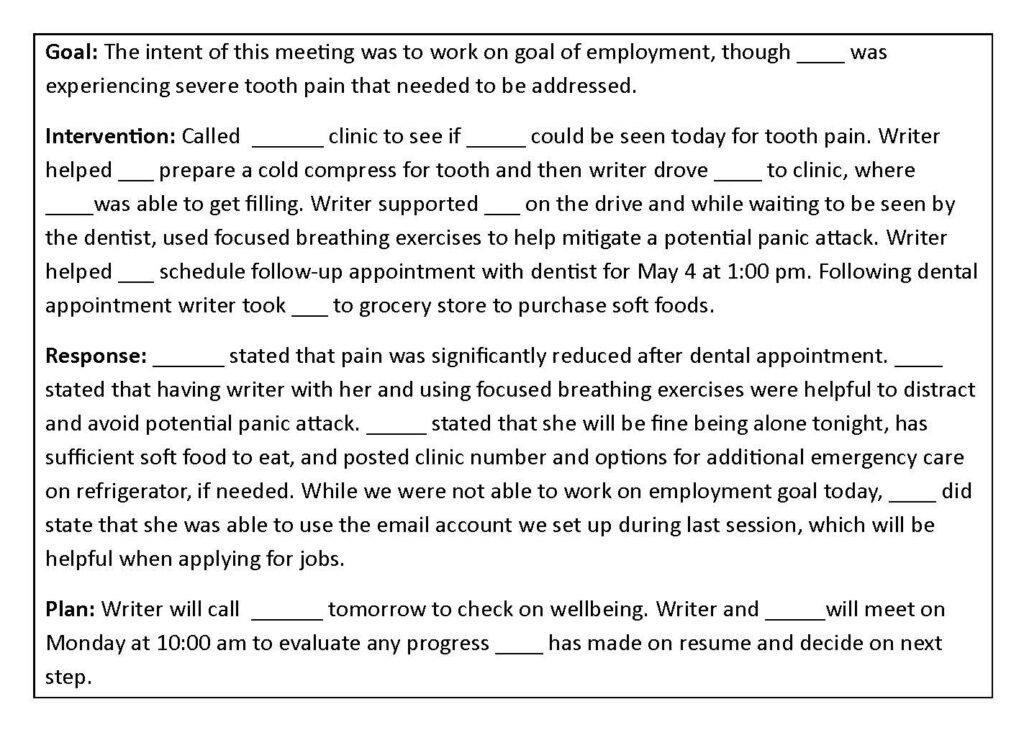
Deviations from goal-oriented work occur frequently in case management services. It’s just the nature of working with people in a world where life challenges exist. Strengths Model Case Management requires us to hold multiple realities in mind when working with people. This includes the fact that all people have meaningful and important values/goals they desire to move toward (even if they haven’t always been successful), AND people experience a multitude of internal and external life challenges along the way that make movement toward these values/goals difficult. In the above example, dental pain was chosen as the challenge, though it could have been a substance use relapse, challenges with intrusive symptoms, a relationship conflict, distressing news the person received, etc. Life happens, and we find a way to work through it. Consider your time for documentation an opportunity to be self-reflective about your practice, to embrace empathy and compassion for the person being served, and to think creatively about how to realign/re-engage with the person around goal-related work.
What if we never get back to the goal?
This happens for a variety of reasons. If we end up writing several progress notes with a goal at the top that we never seem to get to, then it is a perfect time to use a session to re-evaluate the goal and any ambivalence the person might have around it, or even return to the Strengths Assessment and re-look at other areas the person might want to focus efforts on together. That is an advantage of being goal-focused in your note writing because it prompts you to reassess the focus of the helping relationship continuously, and to avoid merely repeating reactive, transactional case management sessions in which the focus is always on the problem of the day.
What if the person and I haven’t arrived at a goal for services yet?
That’s fine. Instead of writing a specific goal in the “goal we plan to work on in the session” section of the template, just write “engagement with person” or “work on identifying a goal for services.” Your interventions should then reflect intentional, purposeful strategies to learn more about the person, discuss the program and options for support, assist with immediate needs, and eventually reach an agreement on goals that will represent outcomes of successful case management services.
Do I use the template if there is a crisis?
If a person is experiencing a crisis (e.g., suicidal ideation, medical emergency, need for hospitalization, sudden loss of housing, risk to personal well-being, etc.), you always focus on resolving the crisis situation rather than the template. The focus should be on the immediate safety of the person, coordinating the care and support the person needs, and communicating with key people who need to be notified related to the person’s care. The template is a helpful tool in most encounters, not a requirement.
Isn’t this the same as collaborative documentation?
process described above involves the worker taking their own notes during a session to organize and improve recall when writing a progress note independently of the person receiving services. Collaborative documentation is the process of working together with the person receiving services to write a progress note at the end of a session. So, while not the same, you can see how using the template in this blog can easily be turned into collaborative documentation just by showing the person what you have written and getting their perspective on what occurred during the session. After getting the person’s feedback on your notes and making any necessary additions/revisions, you can record the official progress note together so they can see what will be entered into their chart. While you will not be able to use collaborative documentation in every session due to time constraints or particularly sensitive situations, I highly recommend it whenever possible. It will save you time doing documentation outside of sessions, and it can also be a therapeutic and empowering way for the person to be involved in the helping process. It can also lead to better engagement, commitment to goals, and shaping how their services are provided.
Conclusion
While it’s impossible to cover every potential situation you might encounter in case management and how to document it, what I hope you see is that the way we approach taking notes during a session can make writing a progress note afterward much more straightforward. Consistent with Strengths Model Case Management, this approach to documentation helps us to be continuously mindful of what is meaningful and important to a person and what they are trying to move toward, even amid the challenges they are experiencing. Merely addressing challenges ceases to be the primary driver of our work. Instead, challenges are addressed in relation to how they impact movement toward the desired goal.
If this approach is appealing to you, I would suggest trying it with one or two people initially to see how it feels. Try it with some people with whom you already have a good relationship and with whom you are already working on a specific goal. Tell them you are trying a new approach to writing more succinct and timely progress notes. Use it as a learning opportunity to find an approach and style that works best for you. Be patient with yourself if it seems clunky at first. As with any behavior change, practice is needed to build muscle memory. From my personal experience and from those whom I have taught this process, it will change the way you view your documentation.